Vaccines are among the most studied tools in modern medicine, yet the biology behind them is often described in shorthand. Drawing on guidance from the World Health Organization (WHO), the US Centers for Disease Control and Prevention (CDC), and the University of Oxford's Vaccine Knowledge Project, here is a plain-language explainer of what a vaccine actually does inside the body.
Training the immune system
The core idea is to teach the immune system to recognize a pathogen without making the person sick. Every vaccine contains an antigen — what the CDC describes as a substance that causes the immune system to begin producing antibodies. Antigens are distinctive molecules, often proteins, found on the surface of a virus or bacterium.
When the immune system encounters an antigen, white blood cells respond. Antibodies are proteins that identify and neutralize foreign substances. Two families of immune cells do much of the heavy lifting: B cells, which produce antibodies that latch onto antigens, and T cells, some of which find and destroy infected cells while others help coordinate the response.
Crucially, the body keeps a record. After the response winds down, the immune system retains long-lived memory B cells and T cells. If the real pathogen appears later, these memory cells recognize it and mount a faster, stronger defense — often before the person feels ill. That is the protection a vaccine is designed to leave behind, achieved without the risks of the disease itself.
The main vaccine types
Different vaccines present the antigen in different ways. According to the WHO and the Vaccine Knowledge Project, the major platforms include:
- Live-attenuated vaccines use a weakened form of the live pathogen. Because it closely resembles a natural infection, this type often produces strong, long-lasting immunity from one or two doses. Measles, mumps and rubella (MMR) and yellow fever vaccines are examples; they are generally not given to people with severely weakened immune systems.
- Inactivated vaccines use a pathogen that has been killed so it cannot replicate. The inactivated polio and hepatitis A vaccines fall into this group and sometimes require boosters.
- Subunit or protein-based vaccines include only specific pieces of the pathogen — such as a key protein — rather than the whole organism. Hepatitis B and human papillomavirus (HPV) vaccines are examples.
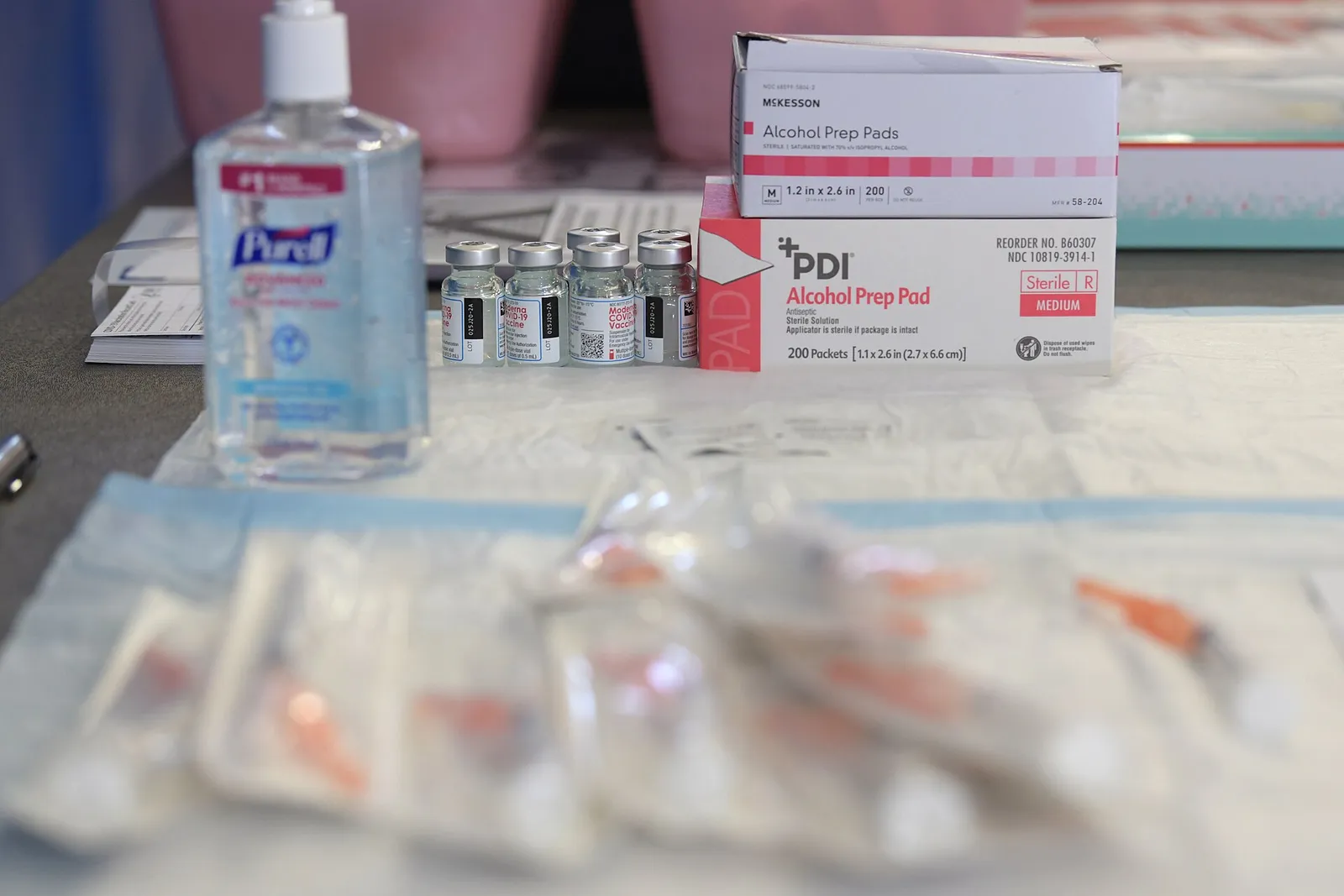
- mRNA vaccines deliver genetic instructions that prompt a person's own cells to make a harmless piece of a pathogen protein, which the immune system then learns to recognize. Some COVID-19 vaccines, including those from Pfizer-BioNTech and Moderna, use this approach. The mRNA does not alter a person's DNA and is broken down by the body.
Herd immunity and protecting the vulnerable
Vaccines do not only protect the individual. When enough people in a community are immune, a contagious pathogen struggles to spread — an effect known as herd immunity or community immunity. The Vaccine Knowledge Project notes this gives indirect protection to vulnerable people such as newborns, elderly people and those too sick to be vaccinated, including some cancer patients and people with compromised immune systems. The share of the population that must be immune to achieve this varies by disease and how easily it spreads.
Testing and safety monitoring
Before approval, vaccines pass through staged clinical trials in volunteers to assess safety and whether they work, followed by regulatory review. After rollout, health authorities continue surveillance to detect rare side effects — systems run by bodies such as the CDC, national regulators and the WHO.
Why availability differs: the Ebola example
A vaccine for one disease does not automatically cover related ones — a point underscored by Ebola. The WHO states there is one licensed and WHO-prequalified vaccine for Ebola virus disease caused by Zaire ebolavirus, the single-dose vaccine Ervebo; a separate two-dose regimen (Zabdeno and Mvabea) also targets that strain. But, the WHO says, "there are no licensed vaccines for Sudan virus disease (SVD) or Bundibugyo virus disease (BVD)." For the Bundibugyo strain — the one behind the current outbreak in the Democratic Republic of Congo — several candidate vaccines are at different stages of development, but none is yet approved.
This explainer is general information, not medical advice. For guidance on specific vaccines, schedules or eligibility, consult a qualified health professional or a national health authority such as the WHO, the CDC or the UK's NHS.